Introduction
Picture this: a patient arrives in the emergency department unconscious. The attending physician pulls up the hospital's EHR system to check for allergies and current medications — but the records are locked behind a system that hasn't communicated with the patient's primary care provider in years. The data exists. It's just inaccessible.
This scenario plays out daily across thousands of US healthcare organizations running on aging infrastructure that was never designed for today's care environment.
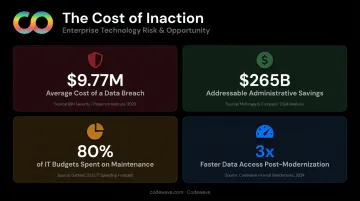
According to IBM's 2024 breach cost analysis, the average healthcare data breach now costs $9.77 million — the highest of any industry. The operational disruption from the Change Healthcare cyberattack alone affected 1 in 3 patient records nationwide and caused 94% of surveyed hospitals to report direct financial impact.
Every year spent on aging infrastructure adds to the risk. Organizations that defer modernization accumulate compounding security exposure, regulatory liability, operational drag, and widening gaps between what patients expect and what outdated systems can deliver.
This article covers what legacy system failure actually costs, which modernization strategies work in practice, the biggest implementation challenges, and a concrete roadmap for getting started.
Key Takeaways
- Legacy healthcare systems create measurable patient safety risks, not just IT headaches
- FHIR API compliance is now a regulatory baseline, not an optional upgrade
- Phased modernization reduces risk while keeping critical services operational
- AI delivers the clearest ROI in administrative workflows, with infrastructure analysis use cases still maturing
- Outcome-based engagement models tie modernization investments directly to measurable results
What Is Healthcare Modernization and Why Do Legacy Systems Fall Short?
Healthcare modernization is the process of upgrading outdated clinical and administrative systems — EHRs, billing platforms, lab tools, patient portals — to be more secure, interoperable, and scalable. It goes far beyond a UI refresh or swapping one software package for another. Understanding what that means in practice starts with identifying what makes a system "legacy" in the first place.
What Makes a System "Legacy"
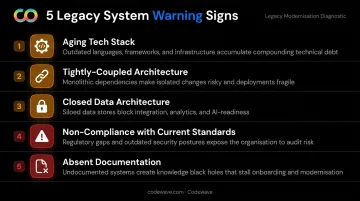
A system doesn't have to be ancient to be a problem. Legacy characteristics include:
- Aging tech stacks — COBOL-based billing systems remain common in payer and claims environments (CMS itself only completed its COBOL-to-Java conversion of 10 Medicare Pricer applications as of January 2022)
- Tightly-coupled architecture — changes to one component risk breaking others with no clean separation
- Closed data architecture — systems that can't expose or consume APIs are locked out of modern data exchange
- Non-compliance with current standards — inability to meet HL7 FHIR R4, USCDI, or ONC certification criteria
- Absent or outdated documentation — no one knows what the system actually does at a code level
Modernization vs. Digital Transformation
These terms get used interchangeably, but the distinction matters.
Modernization targets foundational infrastructure: data pipelines, system architecture, security layers, and compliance controls. Digital transformation builds new patient-facing capabilities — telehealth, remote monitoring, personalization — on top of that modernized base.
Organizations that skip modernization and jump straight to transformation typically discover the gap the hard way: a patient portal goes live, volume spikes, and the underlying data pipeline — still running on decade-old batch processing — can't keep up. The front end looks modern. The infrastructure isn't.
The Real Cost of Running Outdated Healthcare Systems
Security and Compliance Exposure
The numbers here are stark. The AHA reported 386 healthcare cyberattacks as of October 2024. A peer-reviewed 2025 study found ransomware has affected more than half of patients annually since 2020, reaching 69% in 2024.
Older systems typically lack:
- Modern encryption for data at rest and in transit
- Role-based access controls with audit logging
- Automated threat detection or incident response workflows
The result: HIPAA violations, ransomware exposure, and breach costs that dwarf the investment required to modernize.
Patient Safety Risks from Fragmented Data
Data silos across labs, billing, and EHR platforms mean clinicians routinely make decisions with incomplete records. Legacy systems without validation layers or clinical decision-support tools raise the likelihood of:
Data silos across labs, billing, and EHR platforms mean clinicians routinely make decisions with incomplete records. Legacy systems without validation layers or clinical decision-support tools raise the likelihood of:
- Missed or delayed diagnoses from incomplete patient histories
- Medication errors when drug interaction data isn't surfaced at the point of care
- Duplicate procedures ordered because prior results aren't accessible
The emergency department scenario at the start of this article isn't an anomaly. It's a predictable consequence of fragmented infrastructure.
Escalating Maintenance Costs and Skill Scarcity
The GAO has documented that federal IT spends more than $100 billion annually, with about 80% going to operations and maintenance of existing systems. Ten critical legacy systems — aged 8 to 51 years — cost $337 million per year to maintain, largely because the languages they're built in (including COBOL) have a shrinking talent pool.
Healthcare organizations face the same dynamic. IT budgets consumed by patching aging systems aren't available for the clinical data infrastructure that enables value-based care, predictive analytics, or interoperability.
The Opportunity Cost of Inaction
McKinsey estimates that approximately 30 administrative interventions could save US healthcare up to $265 billion annually — including $175 billion from back-office automation and $35 billion from unified payer-provider platforms. Codewave's healthcare infrastructure engagements have produced 3x faster access to healthcare data, up to 40% less reporting time, and maintenance cost reductions of up to 50% post-migration.
Proven Strategies for Upgrading Healthcare Legacy Systems
No single approach fits every system. The right strategy depends on each system's risk level, strategic value, and how tightly it's woven into daily operations.
Encapsulation and API Wrapping
Wrap a legacy system with a modern API or service layer without touching the underlying code. The internal logic stays intact; new platforms — patient portals, analytics tools, telehealth interfaces — interact through standardized interfaces instead.
This is the lowest-risk entry point for most organizations. ONC and CMS policy increasingly centers modernization around standards-based API access — the CMS Interoperability and Patient Access Final Rule requires HL7 FHIR Release 4.0.1 APIs for covered payer interoperability.
Wrapping a legacy payer system to expose FHIR-compliant endpoints can satisfy those regulatory requirements without triggering a full replacement.
Rehosting and Replatforming
- Rehosting (lift-and-shift): Move existing workloads to new infrastructure — typically cloud — with minimal code changes. Best for reducing data center costs and improving reliability. One Codewave healthcare engagement involved migrating clinics from on-premise servers running at 20% utilization to Azure pay-as-you-go infrastructure, freeing up budget for patient engagement programs.
- Replatforming: Migrate to a new platform with targeted optimizations but without a full rewrite. Appropriate when organizations need HIPAA-compliant cloud capabilities — encrypted storage, automated failover, audit logging — that on-premise environments can't provide.
Refactoring and Rebuilding
- Refactoring: Improves internal code structure without changing external behavior. Best when a system's architecture creates performance bottlenecks but the underlying logic is sound.
- Rebuilding: Carries the most risk and should only be considered when a system fundamentally blocks modern care models. Requires the most thorough compliance planning and the longest stabilization runway.
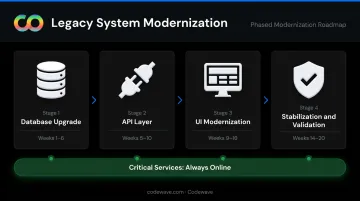
Phased Modernization
For most healthcare organizations, phased modernization is the right default: break the effort into incremental stages — upgrade database, then APIs, then UI — while keeping critical services running. The AMA notes that new EHR go-lives are typically scheduled at least one year after vendor selection, with post-implementation stabilization lasting one to three months. A phased approach maps directly to that timeline — each stage can be validated and stabilized before the next begins.
Retiring and Replacing
Retiring systems that no longer deliver value and replacing them with modern SaaS solutions works well for administrative tools — HR, billing, scheduling — where market-standard options exist. Replacing clinical systems requires thorough data migration planning. Codewave's data migration approach uses automated mapping and predictive validation tools to detect schema mismatches before migration begins, targeting 99.99% data integrity during transitions.
The Biggest Challenges in Healthcare Modernization
Regulatory and Compliance Complexity
Every system change must be evaluated against HIPAA's administrative, physical, and technical safeguard requirements. HHS OCR requires covered entities to conduct a risk analysis of ePHI risks and vulnerabilities — system migrations qualify as changes to the ePHI environment and trigger reassessment.
CMS's information-blocking rules add another layer. Restricting data access to make legacy systems appear more stable than they are exposes organizations to direct regulatory liability.
Codewave embeds HIPAA compliance controls directly into infrastructure design from day one — PHI encryption in transit and at rest, access segregation, audit logging, and incident response playbooks — rather than retrofitting them after go-live.
Clinician Resistance and Adoption Barriers
Peer-reviewed research consistently links EHR-related clerical burden to clinician burnout and turnover. Introducing a new system poorly — without workflow mapping, iterative UX testing, or genuine stakeholder input — often makes the problem worse before it gets better. Human-centered design and early clinician engagement are what separate a successful rollout from one that gets quietly abandoned six months in.
Migration Risk and Operational Continuity
Healthcare systems cannot go offline. A hospital mid-migration isn't like a retail site in maintenance mode — real patients are affected. This is why large-scale, big-bang migrations carry extreme risk in clinical environments.
Proven deployment strategies for clinical environments include:
- Blue-green deployments — run old and new systems in parallel, then switch cleanly
- Canary releases — shift a small percentage of traffic to the new system first, monitor, then expand
- Instant rollback — revert without downtime if unexpected issues surface
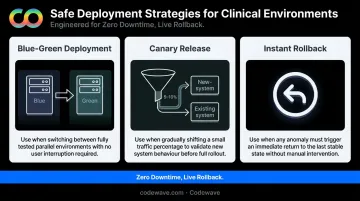
Each approach keeps the existing system live and recoverable throughout the transition.
How AI and Data Integration Are Transforming Healthcare Infrastructure
Interoperability and FHIR Adoption
ONC reported that by 2024, 70% of US hospitals had FHIR app capabilities and 80% enabled inpatient API use — up from 68% in 2021. Two in three hospitals used a FHIR API to enable patient access through apps in 2022, a 12-percentage-point year-over-year increase.
FHIR-compliant APIs don't just satisfy regulatory requirements. They unlock practical integrations across the care continuum:
- Telehealth platforms that pull real-time patient data during virtual visits
- Wearable devices that feed continuous monitoring into clinical workflows
- Population health tools that aggregate data across care settings
Real-Time Data and Predictive Analytics
Legacy systems generate batch reports — often hours or days behind actual clinical events. Modern, integrated infrastructure enables real-time data access that powers genuinely useful analytics. A 2023 systematic review found that machine learning methods using EHR data support early sepsis prediction, a use case where hours matter clinically.
McKinsey's 2025 healthcare generative AI research identifies administrative efficiency, clinical productivity, and patient engagement as the highest-priority AI use cases. Each depends on modernized data infrastructure to function at all.
From Data Silos to Unified Patient Intelligence
That infrastructure dependency becomes clearest at the data layer. Post-modernization, data from EHRs, labs, billing, wearables, and remote monitoring consolidates into a coherent patient view. HHS ASPE notes that value-based care depends fundamentally on easy access to patient records and coordination across practitioners. Organizations that achieve this shift from reactive, transaction-based care to proactive, outcomes-driven models.
Codewave's healthcare platform work focuses on exactly this consolidation: HL7/FHIR integrations across EHR systems, telehealth tools, and patient portals, backed by real-time data pipelines built on Apache Kafka and AWS Lambda for cross-departmental data access.
A Practical Healthcare Modernization Roadmap
Step 1 — Audit and Prioritize
Before touching anything, understand what you have. A comprehensive system inventory should:
- Document every clinical and administrative system, its age, vendor support status, and known vulnerabilities
- Map dependencies between systems to identify what can change safely and in what order
- Flag HIPAA compliance gaps and interoperability limitations against current standards (USCDI, FHIR R4)
- Establish baseline KPIs — uptime, data accuracy, processing speed, error rates — to measure modernization impact
GAO's analysis of critical legacy systems found that the absence of documented modernization plans with clear milestones directly increases risk of cost overruns, delays, and security incidents. The audit is risk management, not bureaucratic overhead. Skip it and you're guessing at dependencies, compliance gaps, and sequencing — all of which become expensive problems mid-project.
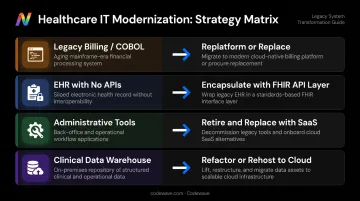
Step 2 — Define Strategy by System
Not every system needs the same approach. Apply the right strategy based on risk level, strategic value, and interdependencies:
| System Type | Likely Strategy |
|---|---|
| Legacy billing (COBOL-based) | Replatform or replace |
| EHR with stable logic, no APIs | Encapsulate with FHIR-compliant API layer |
| Administrative tools (HR, scheduling) | Retire and replace with modern SaaS |
| Clinical data warehouse | Refactor or rehost to HIPAA-compliant cloud |
Governance structure matters here. Establish cross-functional teams — IT, clinical leadership, compliance, operations — before execution begins, not mid-project when decisions get contested.
Step 3 — Partner for Outcomes, Not Just Delivery
Once strategy is defined, execution depends on who you partner with — and how that partnership is structured. When vendors are accountable only for code delivery, not results, modernization projects drift: scope expands, timelines slip, and the organization absorbs the risk.
Outcome-based engagement models change that dynamic. Codewave's ImpactIndex™ ties compensation to measurable business outcomes — system uptime, data processing speed, patient engagement metrics — rather than hours billed. For healthcare organizations working with constrained IT budgets on high-stakes infrastructure, that keeps vendor goals tied to your outcomes, not their billable hours.
Codewave has worked with 400+ businesses across healthcare and adjacent verticals. Documented outcomes include 3x faster healthcare data access, 99.9% uptime post-migration, and maintenance cost reductions of up to 70% through cloud-native modernization.
Frequently Asked Questions
What are the top three trends in healthcare IT right now?
AI-driven diagnostics and clinical decision support, FHIR-based interoperability and data exchange, and the shift to value-based care are reshaping US healthcare infrastructure right now. All three depend on modernized data systems to function effectively.
What is the first step in modernizing a healthcare legacy system?
A comprehensive system audit — inventorying existing platforms, mapping dependencies, identifying security and compliance gaps, and prioritizing systems by risk and business impact. No changes should begin before this baseline is established.
How long does healthcare IT modernization typically take?
Timelines vary widely: a single system can take 3–12 months, while enterprise-wide efforts often span 2–5 years. The AMA notes go-live typically falls at least one year after vendor selection, with 1–3 months of stabilization post-launch.
How do you ensure HIPAA compliance during system modernization?
Conduct a HIPAA risk assessment before any changes begin, maintain audit trails throughout migration, enforce access controls on new systems from day one, and involve compliance teams at every project stage — not just at the end.
What is the difference between healthcare modernization and digital transformation?
Modernization upgrades foundational IT infrastructure: systems, data pipelines, security layers, and compliance controls. Transformation builds new patient-facing capabilities on top of that base — and it needs to come first, because transformation built on legacy infrastructure tends to fail.
Which healthcare legacy systems are modernized first?
EHR and EMR platforms, COBOL-based billing systems, and HL7 v2 messaging interfaces are the most common starting points. They carry the highest operational and security risk, and their modernization unlocks the most downstream value for interoperability and analytics.