Introduction
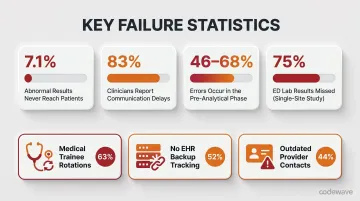
Getting the right lab result to the right provider at the right time is harder than it should be. U.S. clinical labs process 14 billion tests annually — data that drives roughly 70% of all medical decisions — yet 7.1% of clinically significant outpatient results never reach patients, and 83% of clinicians report delays in receiving them.
Fragmented systems, manual handoffs, and siloed Laboratory Information System (LIS) platforms are the root cause. When potassium levels as low as 2.6 mEq/L or hemoglobin A1c as high as 18.9% go uncommunicated, the consequences can be life-threatening.
AI orchestration addresses this directly. It coordinates multiple specialized AI agents — each assigned a distinct task (ingestion, normalization, interpretation, routing, alerting) — into a single automated pipeline. Where traditional workflows depend on manual intervention between steps, an orchestrated system moves every result from analyzer output through standardized formatting to the right provider channel without human handoffs.
This article examines what AI orchestration means in the laboratory context, why traditional workflows fail at scale, how multi-agent architectures function in practice, and what healthcare teams need to implement these systems successfully while meeting HIPAA, CLIA, and ONC interoperability requirements.
TLDR:
- AI orchestration automates the full lab result pipeline — from ingestion through provider delivery — using coordinated specialist agents
- 46–68% of lab errors occur pre-analytically — and 7.1% of abnormal results still never reach patients
- Multi-agent systems handle HL7 v2 and FHIR simultaneously, routing results and triggering critical value alerts automatically
- Successful implementation requires infrastructure assessment, phased rollout, and embedded HIPAA/CLIA compliance from day one
What Is AI Orchestration in Lab Result Integration?
AI orchestration is a coordination framework that directs multiple specialized AI agents through interdependent tasks—in sequence, in parallel, or both—assigning work, managing handoffs, and resolving conflicts across an intelligent lab data workflow. When these agents operate together, the system is called a multi-agent AI system or agentic workflow.
The orchestration layer acts as governance: ensuring agents communicate effectively, prioritize tasks correctly, and never drop a result between handoffs.
How Orchestration Differs from Basic Automation
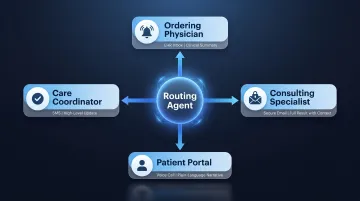
Traditional lab automation follows fixed rules and linear scripts: if Test Result X exceeds Threshold Y, send Alert Z to Provider A. These systems break down when facing complex, multi-format diagnostic data requiring contextual interpretation. AI orchestration involves agents that reason, adapt, and hand off context dynamically—essential when a single result may need simultaneous delivery to an ordering physician, consulting specialist, and patient portal in three different formats.
Scope Within Lab Result Integration
In laboratory environments, orchestration manages the complete journey:
- Raw analyzer output → captured from hematology, chemistry, or molecular platforms
- HL7/FHIR standardization → normalized using LOINC test codes and SNOMED clinical terminology
- Clinical interpretation → analyzed against reference ranges and patient history
- Provider routing → delivered to ordering physicians, specialists, care teams, and patient portals
- Critical alerts → escalated for life-threatening values requiring immediate attention
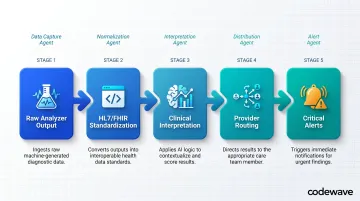
Each step is handled by a dedicated AI agent or module, with the orchestration layer ensuring no result is lost, delayed, or misrouted.
Why Lab Environments Demand Orchestration
Single-use AI tools are designed for narrow tasks. Lab result integration is not narrow. It crosses disciplines like hematology, pathology, and molecular diagnostics; reaches destinations from ordering physicians to patient portals; and operates under layered compliance obligations including HIPAA, CLIA, and state-level regulations.
No single AI model handles that scope. Orchestration does—by coordinating specialized agents across every layer. According to NIST's AI Agent Standards Initiative, autonomous AI agents require industry-led standards for identity, inter-agent communication, and safety protocols. That's precisely the framework orchestration provides for clinical laboratories.
Why Traditional Lab Result Workflows Fall Short
Data Silos Create Communication Gaps
Most laboratories operate with disconnected systems: analyzers feed into an LIS, which may or may not communicate with the EHR, which may or may not notify the responsible provider automatically. Research from Casalino et al. (2009) documented that practices using partial electronic medical records—a mix of paper and electronic systems—had 1.92 times higher failure rates than practices with no EMR and 2.37 times higher rates than those with complete EMRs.
Fragmented digitization is worse than either full paper or full electronic workflows because it creates ambiguity about which system holds the authoritative record.
The scale of the problem is significant. Among more than 266,000 CLIA-certified U.S. laboratories processing 14 billion annual tests, systematic notification failures range from 6.8% to 62% across ambulatory care settings, with one study finding that 62% of abnormal glucose tests received no appropriate follow-up.
Manual Handoffs Don't Scale
Those silos make every result handoff a manual task. When results require routing to multiple providers—a referring physician, a specialist, and a patient portal—staff must manually trigger each communication. This introduces:
- Delays that scale poorly with volume as labs processing tens of thousands of tests daily create bottlenecks
- Transcription errors from manual data entry, which account for a significant portion of the 46-68.2% of lab errors occurring in pre-analytical phases
- Notification failures where up to 75% of emergency department test results were missed in one study
Research by Zimolzak et al. (2021) identified specific failure mechanisms: 63% of staff cited medical trainee rotations as a primary risk, 52% cited lack of EHR backup tracking systems, and 44% identified outdated provider contact information as barriers to timely result communication.
Standards Fragmentation Creates Integration Challenges
Laboratories use a mix of HL7 v2, HL7 FHIR, ASTM, and proprietary formats depending on vendor and implementation era. The NIH National Library of Medicine confirms that HL7 Version 2 remains the most widely used health information exchange standard in the United States — with approximately 95% of healthcare organizations relying on it.
Yet the ONC HTI-1 Final Rule mandates FHIR US Core 6.1.0 adoption by December 31, 2025, putting most organizations on a collision course between their current infrastructure and compliance deadlines.
Without an orchestration layer to normalize these formats in real time, integration becomes a custom-coded patchwork. Each LIS-to-EHR connection requires a bespoke interface, creating what practitioners describe as an "n-to-n" mapping problem — one that breaks whenever any connected system updates.
How AI Orchestration Works: The Multi-Agent Architecture for Lab Results
Ingestion Agent Layer
The first set of agents connects to laboratory analyzers, LIS platforms, and middleware to capture raw result data immediately upon finalization. Rather than periodic polling—which introduces latency—these agents use event-driven triggers. Technologies like Apache Kafka enable real-time streaming that processes HL7 v2 messages with minimal lag.
Astrana Health documented deploying Kafka combined with AWS Lambdas for real-time healthcare event streaming, contrasting sharply with the industry-standard 30-90 day lag typical of batch-processed claims data.
Normalization and Validation Agent
Once raw data is captured, this agent:
- Maps results to standardized formats: HL7 FHIR DiagnosticReport resources, LOINC codes for test identifiers (covering over 100,000 codes across 193 countries), and SNOMED CT for clinical terminology
- Validates completeness: Checks for missing fields, invalid reference ranges, or formatting errors
- Flags anomalies: Identifies results requiring human review before downstream processing
This normalization step is critical because ONC certification requires LOINC for representing laboratory test names in certified EHRs, and FHIR US Core 6.1.0 mandates specific resource formatting.
With results standardized and validated, the next agent layer moves from formatting to clinical meaning.
Interpretation Agent
This AI layer analyzes normalized results against:
- Clinical reference ranges appropriate to patient demographics and test methodology
- Patient history where available via EHR integration
- Evidence-based guidelines to generate structured narrative summaries, differential insights, and follow-up recommendations
The interpretation agent reduces clinician workload by transforming raw numeric results into contextualized clinical information, highlighting values requiring attention and suggesting potential next steps.
Intelligent Routing Agent
This agent determines which providers, care teams, or patient-facing channels should receive the result, in what format, and through which delivery mechanism:
- EHR alerts for ordering physicians requiring immediate action
- Secure messaging for consulting specialists who need context but not real-time alerts
- Patient portal notifications with patient-friendly narrative summaries
- Voice AI calls for critical values requiring immediate acknowledgment
The routing agent can deliver the same result to multiple recipients simultaneously without duplication errors, with each recipient receiving a format and level of detail appropriate to their role.
Critical Value Alerting Agent
For abnormal or life-threatening results—sepsis markers, critical electrolyte levels, severe anemia—a dedicated agent applies configurable threshold rules to trigger priority alerts. CLIA regulation 42 CFR 493.1291(g) requires laboratories to "immediately alert" ordering providers when results indicate "imminently life-threatening" conditions. The Joint Commission NPSG.02.03.01, effective January 2026, mandates that laboratory programs report critical results "on a timely basis" with documented procedures and timeliness evaluation.
Critical value agents:
- Bypass standard delivery queues to ensure immediate notification
- Escalate through direct channels to responsible clinicians
- Maintain audit trails for compliance and quality review
- Require acknowledgment to confirm receipt and understanding
Feedback and Audit Loop
The orchestration layer logs every agent action, result state, and delivery confirmation—creating a complete chain of custody for regulatory compliance. This audit trail satisfies:
- HIPAA requirements for tracking access to electronic protected health information
- CLIA mandates for documenting result reporting and error correction
- ONC HTI-1 transparency requirements for AI algorithm decision-making
When a delivery fails or an agent underperforms, the audit loop surfaces the issue before it reaches the clinician—turning compliance infrastructure into an active quality control mechanism.
Key Capabilities That Make AI-Orchestrated Lab Integration Work
Interoperability by Design
Effective orchestration must natively support both HL7 FHIR RESTful APIs (anticipated for 84% adoption increase) and legacy HL7 v2 messaging (used by 95% of U.S. healthcare organizations). This dual-standard support enables integration with modern cloud-based EHRs and legacy on-premises LIS platforms without requiring labs to replace existing infrastructure, a practical necessity given the capital already invested in current systems.
Two standards anchor the terminology layer:
- LOINC: Covers standardized test identification for at least 98% of a typical lab's test catalog
- SNOMED CT: Enables codified clinical terminology exchange across systems
The orchestration layer handles format translation between these standards, mapping v2 message segments to FHIR resources without manual intervention.
Multi-Provider, Multi-Channel Delivery
The system must push finalized, interpreted results to multiple providers simultaneously:
- Ordering physician receives a clinical summary with actionable recommendations
- Consulting specialist gets the full result with relevant patient context
- Care coordinator sees a high-level status update for care plan adjustments
- Patient portal displays a plain-language narrative, free of clinical jargon
Each recipient receives a format and level of detail appropriate to their role, delivered through their preferred channel: EHR inbox, secure email, SMS alert, or voice call.
Scalability and Real-Time Processing
Laboratories processing tens of thousands of tests daily require orchestration architecture that handles concurrent agent execution without bottlenecks. Quest Diagnostics, the largest independent U.S. clinical laboratory, processes approximately 156 million test requisitions annually, while LabCorp handles approximately 2.5 million specimens per day. At this scale, even milliseconds of latency per transaction compound into hours of cumulative throughput loss across daily volume.
Enterprise deployments require high-throughput message processing infrastructure, distributed agent execution, and elastic scaling to accommodate daily volume fluctuations without degrading performance.
Exception Handling and Human-in-the-Loop Escalation
Orchestration should not be fully autonomous for edge cases. When an agent encounters:
- Ambiguous data that doesn't map cleanly to standardized codes
- Failed normalization due to unexpected format variations
- High-risk results requiring clinical judgment beyond threshold rules
The system should route to a human reviewer with full context preserved, displaying the original data, the agent's interpretation attempt, and the specific reason for escalation. This prevents silent failures or proceeding with incomplete information while maintaining workflow efficiency for the 95%+ of results that process automatically.
Implementing AI Orchestration: What Healthcare Teams Need to Know
Infrastructure and Readiness Assessment
Before deploying an orchestration layer, teams should:
Audit existing data flows:
- Identify all result-generating systems (analyzers, middleware, LIS platforms)
- Map all downstream consumers (EHRs, patient portals, referring physician systems, specialists)
- Document current integration methods (HL7 v2 interfaces, FHIR APIs, manual processes, fax)
Evaluate HL7/FHIR maturity:
- Determine which systems support FHIR APIs vs. legacy v2 messaging
- Assess API documentation quality and availability
- Identify gaps requiring custom interface development
Confirm event-driven capabilities:
- Verify whether LIS/EHR platforms expose real-time event hooks for result finalization
- Determine whether current infrastructure supports streaming architecture
- Assess network bandwidth and latency for real-time messaging
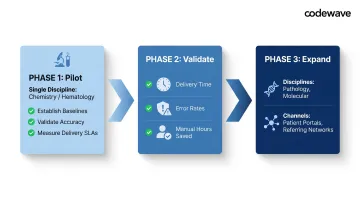
Phased Rollout Approach
Begin with a single high-volume lab discipline—clinical chemistry or hematology—where:
- Test volumes are sufficient to demonstrate value but manageable for pilot validation
- Result types are relatively standardized with clear reference ranges
- Provider routing patterns are well-established
Establish performance baselines:
- Current result delivery time from finalization to provider notification
- Error rates for misrouted, delayed, or lost results
- Manual processing hours per day spent on result communication
Validate accuracy and delivery SLAs:
- Confirm normalization accuracy against manual coding
- Measure delivery latency for routine and critical results
- Track provider acknowledgment rates and feedback
Expand incrementally to additional disciplines (pathology, molecular diagnostics) and provider channels (patient portals, referring physician networks) after validating the initial implementation. Working with an experienced healthcare AI implementation partner during this phase helps teams navigate common integration pitfalls—particularly around real-time streaming architecture and normalization accuracy—before scaling to additional departments.
Compliance and Governance Requirements
The orchestration layer must embed regulatory compliance from day one:
HIPAA technical safeguards (45 CFR 164.312):
- Access control: Unique user identification and role-based authorization for each agent
- Audit controls: Hardware, software, and procedural mechanisms recording all system activity
- Transmission security: TLS encryption for all data transmitted between agents and external systems
CLIA requirements (42 CFR 493.1291):
- Accurate, reliable, timely result delivery from data entry to final destination
- Immediate alerting for life-threatening values
- Prompt error correction with retention of original and corrected reports
ONC HTI-1 requirements:
- AI algorithm transparency enabling clinical users to assess fairness, appropriateness, validity, effectiveness, and safety
- Auditable events and reports for all AI-driven decision-making
- FHIR US Core 6.1.0 support by December 31, 2025
Build these controls into the architecture from the start. Organizations that retrofit compliance after deployment face significantly higher remediation costs and audit exposure. Document controls, run regular audits, and keep audit trails ready for regulatory inspections.
Frequently Asked Questions
What is AI orchestration (what do you call multiple AI agents working together)?
Multiple AI agents working together are called a multi-agent AI system or agentic workflow. AI orchestration is the coordination layer that directs these agents—assigning tasks, managing handoffs, and resolving conflicts—so they function as a unified, intelligent pipeline rather than isolated tools that require manual integration.
How do you orchestrate multiple AI agents to deliver lab results to multiple providers?
An orchestration controller receives the finalized result event, triggers the routing agent with a provider manifest (ordering physician, specialists, patient portal), and dispatches simultaneous, role-appropriate delivery through each configured channel. Delivery confirmations are fed back to the audit log to ensure no recipient is missed and compliance requirements are satisfied.
What interoperability standards does AI orchestration use for lab result exchange?
AI orchestration uses HL7 FHIR (DiagnosticReport resources, RESTful APIs) as the modern standard, alongside HL7 v2 for legacy system compatibility. LOINC codes standardize test identification, while SNOMED CT provides clinical terminology. The orchestration layer handles format translation between these standards automatically.
How does AI orchestration handle critical or abnormal lab results?
A dedicated alerting agent applies configurable clinical thresholds to flag critical values, bypasses standard delivery queues, and triggers priority notifications directly to the responsible clinician. Full audit trails are maintained for compliance with CLIA immediate alerting requirements and Joint Commission timeliness mandates, with acknowledgment tracking to confirm receipt.
Is AI orchestration for lab results HIPAA compliant?
HIPAA compliance requires TLS encryption in transit, AES-256 encryption at rest, role-based access controls, and comprehensive audit logging of every agent action per 45 CFR 164.312 technical safeguards. Minimum necessary data handling principles apply to all agent interactions and result delivery events.
What existing systems need to integrate for AI orchestration to work effectively?
The core systems are laboratory analyzers and middleware, the Laboratory Information System (LIS), the Electronic Health Record (EHR), and patient-facing portals or communication channels. The orchestration layer sits as the integration hub, using event-driven triggers to capture results at finalization and route them to the right destination.
Ready to eliminate lab result delays? Codewave has helped healthcare organizations achieve 90% fewer data errors and 3× faster processing through custom AI orchestration implementations. Contact us to discuss your lab integration challenges and explore what a multi-agent system can deliver for your workflows.