Introduction
US healthcare systems face a compounding problem. Chronic diseases drive 90% of the $5.3 trillion in annual healthcare costs, while HRSA projects a shortage of more than 141,000 physicians by 2038. At the same time, 49% of healthcare workers report burnout, and hospitals absorbed over $42.5 billion in additional labor costs between 2021 and 2023.
Monitoring patients only during scheduled visits was never a complete solution. Between appointments — especially for patients with heart failure, diabetes, or COPD — is precisely when disease control breaks down and costly deterioration occurs.
AI-powered remote patient monitoring (RPM) is increasingly central to how health systems are responding. This article examines what it actually delivers: earlier clinical intervention, tighter chronic disease control, and measurable reductions in hospitalizations and costs — and what health systems risk when they delay adoption.
Key Takeaways
- AI RPM converts continuous biometric data into actionable clinical intelligence, enabling intervention before deterioration reaches emergency thresholds
- Early detection via machine learning has reduced first heart failure hospitalization risk by 22% in monitored populations
- Remote glucose monitoring is associated with a 23% higher rate of patients reaching target HbA1c control
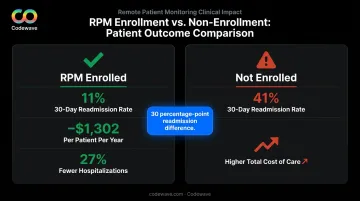
- RPM programs have cut 30-day readmission rates from 41% to 11% in some cohorts, avoiding the average $16,300 cost per readmission
- AI RPM shifts care from reactive to proactive, reducing staff burden, lowering readmission penalties, and protecting long-term operational margins
What Is AI Remote Patient Monitoring?
CMS defines RPM as patients collecting health data through connected devices that automatically transmit information to a provider. AI RPM extends this further: machine learning analyzes the continuous data stream to detect patterns, predict deterioration risk, and trigger alerts before a clinical event becomes apparent to a clinician.
The devices involved are practical and widely used:
- Blood pressure cuffs for hypertension management
- Continuous glucose monitors and connected meters for diabetes
- Pulse oximeters for COPD and respiratory conditions
- Weight scales and biosensors for heart failure decompensation monitoring
- ECG patches for cardiac arrhythmia and risk detection
Where AI RPM Is Applied
AI RPM is most commonly deployed in:
- Chronic disease management (heart failure, diabetes, hypertension, COPD)
- Post-discharge monitoring for high-risk patients
- Post-surgical recovery oversight
- Oncology support and clinical trial monitoring
The goal across all these settings is faster, more informed clinical decisions — and fewer adverse events. Adoption numbers bear this out: Medicare RPM services grew from 160,595 in 2019 to over 5.5 million in 2023, with payments rising from $8.5 million to $255 million over the same period.
Key Advantages of AI Remote Patient Monitoring
The three advantages below are assessed on dimensions health systems actually track: early intervention rates, readmission rates, cost per patient, staff efficiency, and disease control metrics.
Advantage 1: Proactive Early Detection and Predictive Alerting
Between visits, patient status changes. The question is whether the care team finds out in time to intervene — or in the emergency department.
AI RPM answers that question by continuously analyzing incoming biometric streams against each patient's individual baseline. Not against a population average. Against their normal. When heart rate variability shifts subtly or blood pressure patterns change over 48 hours, machine learning models flag the anomaly and push real-time alerts to clinical staff.
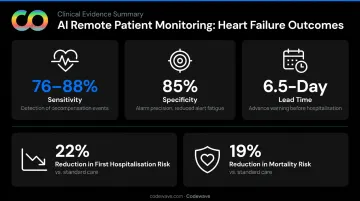
The LINK-HF multicenter study demonstrated this with precision: an AI-analyzed multisensor chest patch detected heart failure hospitalization precursors with 76% to 88% sensitivity and 85% specificity, with a median 6.5-day lead time before the event. That's nearly a week of intervention window that simply doesn't exist under episodic monitoring.
A 2025 meta-analysis of 41 studies and 16,312 patients found RPM reduced the risk of first heart failure hospitalization by 22% (OR 0.78) and mortality risk by 19% (OR 0.81). In a smaller prospective cohort of high-risk post-discharge patients, 3-month hospitalizations dropped from 0.45 to 0.19 per patient and ED visits from 0.48 to 0.06.
KPIs impacted:
- Hospital admission rates
- ED utilization
- Time-to-intervention
- Mortality rates for high-risk patients
- Clinical alarm response times
When this matters most: Early detection has the highest clinical return for high-acuity populations — post-surgical patients, those with decompensating chronic conditions, and patients in rural settings where emergency response time is a critical variable.
Worth noting: predictive alerts only reduce hospitalizations when care teams have defined escalation protocols and coverage to act on them. Detection without response infrastructure doesn't prevent admissions.
Advantage 2: Continuous, AI-Driven Chronic Disease Management
For patients managing diabetes, hypertension, heart failure, or COPD, the gap between clinic visits is where disease control erodes. A patient who leaves an appointment with well-controlled blood pressure may spend the next six weeks in a deteriorating trajectory that no one sees until the next visit — or until an acute event forces the issue.
AI RPM addresses this directly. Algorithms analyze daily biometric trends and flag care team members when readings move outside personalized thresholds — enabling medication titration, lifestyle counseling, or escalation without requiring an in-person visit.
The clinical evidence is specific:
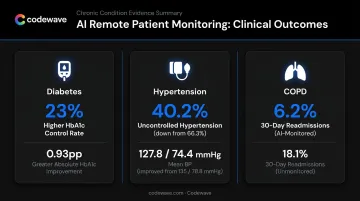
Diabetes: In a study of 35,958 newly diagnosed Type 2 diabetes patients, remote glucose monitoring users had a 23% higher rate of reaching HbA1c ≤8%, with 0.93 percentage-point greater absolute HbA1c improvement among patients who started above 8%.
Hypertension: In a retrospective cohort of 6,595 RPM patients, blood pressure improved from 135/78.8 to 127.8/74.4 mmHg. Among stage 2 patients, the improvement was 16.7/9.0 mmHg. Uncontrolled hypertension fell from 66.3% to 40.2%.
COPD: A 2024 systematic review found COPD telemonitoring programs with substantially lower readmission rates — one study reported 6.2% vs. 18.1% for 30-day all-cause readmissions in monitored versus unmonitored patients.
KPIs impacted:
- HbA1c levels and glycemic control rates
- Systolic blood pressure and hypertension control rates
- 30-day COPD readmission rates
- Medication adherence rates
- Care team time per patient interaction
When this matters most: This advantage has the highest impact in health systems managing large panels of chronically ill patients, value-based care contracts, or populations with limited access to frequent in-person visits — where continuous oversight directly ties to quality benchmarks and reimbursement performance.
Advantage 3: Reduced Hospital Readmissions and Lower Care Costs
Hospital readmissions represent one of the most controllable cost drivers in US healthcare — and one of the most penalized. CMS caps Hospital Readmissions Reduction Program (HRRP) payment reductions at 3% for conditions including heart failure, COPD, pneumonia, and AMI.
The numbers make the exposure concrete. AHRQ data shows the average 30-day readmission cost was $16,300 in 2020 — higher than the $14,500 average index admission cost. The national 30-day all-cause readmission rate sat at 13.9 per 100 index admissions from 2016 to 2020.
AI RPM targets this directly. Post-discharge patients are monitored continuously through connected devices. AI identifies early signs of deterioration — weight gain in heart failure patients, oxygen desaturation in COPD patients, blood pressure spikes in cardiac patients — and triggers care team outreach before readmission becomes necessary.
The outcomes data is consistent: one retrospective analysis found 11% 30-day all-cause readmissions in enrolled RPM patients versus 41% in non-enrolled patients — a 30 percentage-point absolute difference. A separate analysis of 5,872 Medicare chronic disease patients found -$1,302 per patient per year in total cost of care and 27% fewer hospitalizations.
KPIs impacted:
- 30-day readmission rates
- Cost per patient episode
- Bed utilization rates
- Care coordination efficiency
- Total annual cost of care per chronic patient
Highest-impact settings: Systems operating under value-based care or bundled payment models, where readmission penalties directly affect revenue. Also high-volume post-acute settings where patient volume makes manual follow-up operationally infeasible.
What Happens When AI RPM Is Missing or Ignored
Healthcare systems that rely on episodic, visit-based monitoring absorb specific, quantifiable costs:
Clinical consequences:
- Deterioration is identified only at emergency thresholds, requiring higher-acuity and more expensive interventions
- Chronic disease patients cycle through poorly controlled periods that accumulate into costly acute events
- High-risk patients in rural areas have narrower intervention windows when problems surface late
Operational consequences:
- Care teams face administrative overload from unstructured patient data and reactive crisis management
- Alert fatigue increases as manual triage replaces systematic monitoring
- Time spent in crisis mode crowds out planned, preventive care
Financial consequences:
- Readmission penalties accumulate under HRRP for covered conditions
- Staff turnover rises under sustained workload pressure — and AHA data shows hospital labor costs already increased by $42.5 billion between 2021 and 2023
- Health systems lose ground on quality benchmarks that govern reimbursement under value-based contracts
These aren't edge-case failures. Each gap compounds the next — missed early signals drive emergency interventions, which drive burnout, which drive turnover, which widen the monitoring gaps further. AI RPM breaks that cycle at the source.
How to Get the Most Value from AI Remote Patient Monitoring
AI RPM doesn't deliver uniform returns across all patient populations. The highest clinical and financial value concentrates in patients where the intervention window is short and continuous monitoring prevents the most expensive outcomes: high-risk chronically ill patients, post-discharge cohorts, and those managing conditions covered under HRRP.
Practical steps for maximizing RPM impact:
- Stratify before you deploy — Enroll patients based on clinical risk criteria (diagnosis, comorbidity burden, recent hospitalization history) rather than convenience or device availability
- Map alerts to response protocols — AI-generated signals only reduce adverse events when care teams have defined, staffed escalation pathways to act on them
- Integrate into EHR workflows — RPM data flowing into clinical systems without friction means clinicians act on insights rather than hunting for them across platforms
- Train care teams to trust the signals — AI-generated alerts must be treated as primary clinical inputs, not supplementary data to review when time allows
- Track condition-specific KPIs — Monitor HbA1c improvement, blood pressure control rates, and 30-day readmission rates by cohort to measure program performance and refine enrollment criteria
For health systems building or customizing RPM infrastructure, the technical architecture determines how reliably the system performs at scale. Codewave's healthcare technology practice helps organizations design monitoring systems that integrate with existing clinical workflows — using TensorFlow for real-time inference and Apache Kafka for continuous data streaming. HIPAA-compliant architecture, including end-to-end encryption, role-based access controls, and full audit logging, is built in from the start.
Conclusion
AI remote patient monitoring delivers value through three outcomes that build on each other:
- Earlier clinical intervention — catching deterioration before it becomes an emergency
- Tighter chronic disease control between visits, reducing the frequency of acute events
- Lower system-wide costs driven by fewer avoidable hospitalizations and readmissions
Earlier detection prevents the acute events that drive readmissions. Better chronic disease control reduces how often those events occur in the first place.
AI RPM should be treated as an ongoing clinical practice, not a technology project with a go-live date. Its advantages grow as models learn from real patient data, as workflows mature around acting on AI-generated signals, and as care teams build confidence in the system's outputs. Health systems that commit to it as infrastructure — rather than a one-time pilot — are the ones that see these gains compound over time.
Frequently Asked Questions
How is AI used in remote patient monitoring?
AI analyzes continuous streams of biometric data from connected devices to detect patterns, predict deterioration risk, generate real-time alerts, and personalize care recommendations. This lets care teams intervene before conditions escalate — often days earlier than traditional episodic monitoring allows.
What conditions benefit most from AI-powered remote patient monitoring?
AI RPM works best for chronic, high-variability conditions: heart failure, diabetes, hypertension, COPD, and post-surgical recovery. Continuous monitoring fills the gaps between clinic visits, preventing acute exacerbations that drive emergency care and readmissions.
How much does Medicare pay for RPM?
Medicare reimburses RPM services under CPT codes 99453 (setup), 99454 (device supply), 99457, and 99458 (treatment management). Applicable monitoring codes require at least 16 days of data collection per 30-day period. Verify current payment rates directly using the CMS Physician Fee Schedule Look-Up Tool or consult a billing specialist, as rates vary by locality and facility setting.
Does HIPAA allow AI?
HIPAA does not prohibit AI. It requires that any AI system handling protected health information (PHI) comply with HIPAA's Privacy and Security Rules — including data encryption, role-based access controls, audit logging, and business associate agreements (BAAs) with AI vendors. Meeting these requirements is an implementation challenge, not a reason to avoid AI.
What is the most popular remote patient monitoring?
Cardiac monitoring (ECG, blood pressure) and glucose monitoring for diabetic patients represent the most widely adopted RPM applications in the US. Pulse oximetry expanded rapidly after COVID-19 and remains in strong demand for COPD and post-discharge respiratory monitoring.
How does AI RPM reduce hospital readmissions?
AI RPM detects early signs of post-discharge deterioration — such as weight gain in heart failure patients or oxygen desaturation in COPD patients — and triggers timely care team outreach before the issue requires re-hospitalization. One program reported 11% readmissions in enrolled patients versus 41% in non-enrolled patients — a stark illustration of what earlier intervention can achieve.